

Table of Contents
Characterization and injection of Car-T cells
The median lentiviral CAR gene migration efficiency was 56.8% (range, 6.2-78.1%) for all CAR-T cells manufactured. All patients were administered fludarabine and cyclophosphamide (FC) regimen (fludarabine 30 mg/m2/d days -4 to -2 and cyclophosphamide 500 mg/m2/d run one distance in the range of motor vehicle hcart19 for lymph node chemotherapy. 0.83–3.19) x 106 CAR-T cells/kg. Furthermore, we evaluated the expression levels of CD4, CD8, CD45RA, and CD62L in CAR-T products using flow cytometry. No significant differences in CAR-T characteristics were observed between patients who achieved CR and patients in the non-CR group (Supplementary Fig. 1).
Patient characteristics
Between August 23, 2020 and June 12, 2023, 33 patients with R/R B-NHL were screened for eligibility. Of these, six patients did not meet the inclusion criteria (Figure 1A): 3 were 75 years or older, 1 had previously received CAR-T cell injection, 1 had severe infection at screening, and 1 had elevated serum creanaine levels. Additionally, one patient withdraws from the study due to disease progression after leukocytosis. Finally, a total of 26 patients received successful HCART19 treatment and the clinical characteristics of baseline are detailed in Table 1.
Patient registration, treatment, and follow-up (a). Patient responses in the efficacy analysis set (b). Overall survival (OS) (C) and progression-free survival (PFS) (D) (D) (D) in all patients receiving HCART19 infusion.
Median age was 61.5 (range, 28-72), with 15 (57.7%) patients being male. Twenty-four (92.3%) patients were diagnosed with diffuse large cell lymphoma (DLBCL) with B-cell lymphoblastic lymphoma (B-LBL). The majority of patients (n = 23, 88.5%) were in stage III-IV, and three (11.5%) were in stage I-II. The median number of previous lines of chemotherapy was 4 (range, 2-9), with 14 (53.8%) patients receiving 4 lines of chemotherapy prior to CAR-T cell injection. Two patients had undergone previous AUTO-HSCT. Of the patients with DLBCL (n = 24), 16 (66.7%) had an International Prognostic Index (IPI) score ≥3 and 8 (33.3%) had an IPI score <3. Of all patients, 4 (15.4%) had detectable genetic mutations, including 2 containing the TP53 mutation, 1 with the Notch2 mutation, and 1 containing the PXA5 mutation.
Of the 26 patients, 19 (73.1%) had developed BCA prior to HCART19 injection. Before HCART19 infusion, the median CD19+ lymphocytes in the patient's peripheral blood or bone marrow was 0.77% (range, 0.02-78.03%).
Safety
The most common treatment-pervasive adverse events in all grades included lymphopenia (26/26, 100%), pyrexia (23/26, 88.5%), anemia (22/26, 84.6%), CRS (22/26, 84.6%), and Nethropenia (21/26, 80.8%). The most common severe adverse events (grade 3 or higher) were lymphopenia (26/26,100%), anemia (16/26, 61.5%), thrombocytopenia (13/26, 50.0%), and neutropenia (7/26, 26.9%). Other treatment-related toxicities are primarily low grade, including increased aspartate aminotransferase (AST) (10/26, 38.5%), increased alanine aminotransferase (ALT) (6/26, 23.1%), increased serum crectinin (5/26, 19.2%), and increased virbin. The infection occurred in 16 (61.5%) patients, and chest CT scans in 13 (50.0%) patients showed signs of inflammation. Two patients were tested positive in the T-spot assay. One patient received quadrature antituberculosis therapy, but evidence of tuberculosis infection in another was inconclusive. Two patients had asymptomatic cytomegalovirus (CMV) activation and received ganticlovir for treatment.
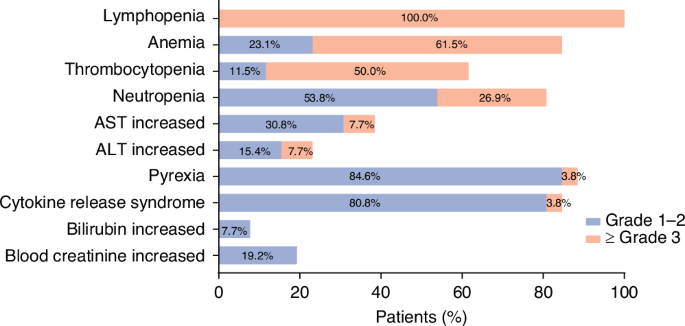
AST aspartate aminotransferase, ALT alanine aminotransferase.
Grade CRS occurred in 22 (84.6%) patients, including 14 patients with Grade 1 CRS, 7 patients with Grade 2 CRS, and 14 patients with Grade 3 CRS. The major symptoms observed in the majority of patients who encountered CRS included fever. No CRS-related deaths occurred. Median and duration of onset of CR after injection were 3 days (range, 1-10) and 7 days (range, 1-47), respectively. All CRS episodes were effectively managed following traditional CRS interventions, with two patients receiving glucocorticoids and three receiving tricimab and glucocorticoids. However, no significant differences were observed between patients with grade 2-3 CRS and grade CRS (P>0.05) at peak levels of serum C-reactive protein (CRP), lactate dehydrogenase (LDH), ferritin, and cytokines (IL-2, IL-4, IL-6, IL-6, etc.) (P>0.05). No patients had ICAN. Patient 9 experienced mild headaches and dizziness. This was resolved with betahistine three times a day.
Effectiveness and follow-up
Twenty-six patients who received HCART19 infusion were included in the efficacy analysis. Twenty-one patients (80.8%) achieved objective responses on day 28 assessments including day 18 CRS and 3 (11.5%) PRS (Figure 1B). Five (19.2%) patients did not obtain a response (NR) including two with stable disease and two with progressive disease.
The median follow-up was 20.3 months (range, 1.1-45.5), with 77.8% (14/18) of CR patients remaining CR, and 22.2% (4/18) of CR patients recurring (Figure 3). Of the three PR patients and five NR patients, all suffered from disease progression, all (except one NR patient) eventually died. Patient 23 received serial CD22 CAR-T cell injections 3.8 months after HCART19 injection, but recurred at 9.5 months. Estimated OS and PFS were 65.8% (95% CI, 49.1% to 88.2%) and 54.8% (95% CI, 38.1% to 78.7%), and 57.0% (95% CI, 40.0% to 81.2%) and 50.5% (95% CI, 34.0%) over the course of 1c and d). Median OS and PFS were 20.3 months (range, 1.1-45.5) and 11.3 months (range, 0.9-45.5), respectively. Twelve individuals (12/26, 46.2%) died during this study: 9 died of recurrence or progression of the disease, one patient (patient 3) died of progression of hepatocellular carcinoma, and two patients (patient 20 and patient 23) died of respiratory failure.
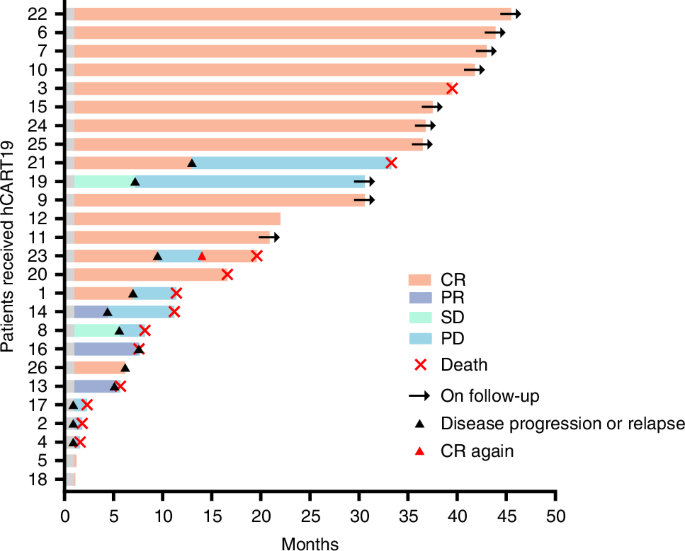
Clinical results for patients during follow-up.
In the analysis of all patients administered with HCART19, the factors included in this study were not significantly associated with treatment response (Supplementary Figure 3). In multivariate analysis, low levels of LDH (LDH level <300 U/L, P = 0.018) before CAR-T cell injection were significantly correlated with better PF (Supplementary Fig. 4 and Supplementary Table 2). However, both univariate and multivariate analyses showed that the factors had no significant correlation with OS (Supplementary Table 3).
Car-T cell proliferation and persistence
CD19 CAR-T cells in peripheral blood were detected by flow cytometry after cell injection (Fig. 4). The median peak percentage of CD19 CAR-T cells proliferation was 44.38% (range, 7.06-83.00%). Median peak number of circulating CD19 CAR-T cells was 220.63 cells/µL (range, 20.16–2651.39 cells/µL), with median to median AUC0-28 at 1990.0 (range, 132.4–18971.0)/µL × for 13 (range, 9–30) days. There were no statistically significant differences observed between CR and non-CR patients with peak CAR-T cells (P = 0.238) and AUC0-28 (P = 0.367). However, both peak CAR-T cells (P = 0.019) and AUC0-28 (P = 0.041) increased significantly among patients experiencing grade 2-3 CRS compared to those with grade 0-1 CRS. Reduced CAR-T cell proliferation occurred in most patients at 28 days. CAR-T cells expansion at day 10 assessment after HCART19 injection in patients with grade 2-3 CRS was significantly higher than in patients with grade 0-1 CRS (353.2 vs. 61.7 cells/µL, P = 0.047). However, CAR-T cells expansion at other evaluation dates in patients with grade 2-3 CRS was higher, but not more significant than those with grade 0-1 CRS (P>0.05) (Fig. 4B). Furthermore, the expansion of CAR-T cells in patients who recurred or did not respond was not significantly different from those in patients who had a continuous response (P>0.05) (Fig. 4C).
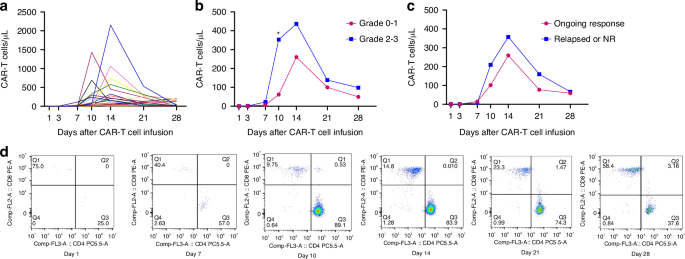
CAR-T cells expansion in all patients between day 0 and day 28 (a). CAR-T cell counts were after peripheral blood injection of patients with grades 0-1 CRS and grades 2-3 CRS (B). The number of CAR-T cells had a post-injection of peripheral blood in patients who relapsed or acquired or acquired a response (NR) and an ongoing response (C). Representative flow cytometric analysis of peripheral blood samples collected from one patient with ongoing CR(D). symbol
It shows p <0.05, but does not use asterisks for non-significant comparisons.
All patients developed BCA after infusion of HCART19. Median duration of BCA was 1.8 months (range, 0.5-23.6) after perfusion. Six patients showed symptoms of BCA, five of whom remained in sustained remission after HCART19 infusion, showing durable persistence of HCART19 cells. Twelve (46.2%) patients were able to detect CAR-T cells for at least 50 days based on peripheral blood flow cytometry analysis. Eight (30.8%) patients made CAR-T cells detectable for at least 3 months. One patient (patient 3) showed long-term Car-T cell persistence in vivo, indicating that CAR-T cells were still detectable in peripheral blood 31.4 months after perfusion.
