
To determine suitability for organ transplantation after cardiovascular death, it is necessary to determine whether a potential donor has undergone LST without clear medical benefit. This process includes securing patient and family consent for organ donation, withdrawal of life support, declaration of cardiovascular death through well-defined protocols, and procurement of organs for transplantation. At each step, ethical considerations must be carefully identified and addressed. Notably, this study did not provide a detailed examination of ethical issues among participants. However, confirming the wishes of patients and their families for organ transplantation was rather simple.
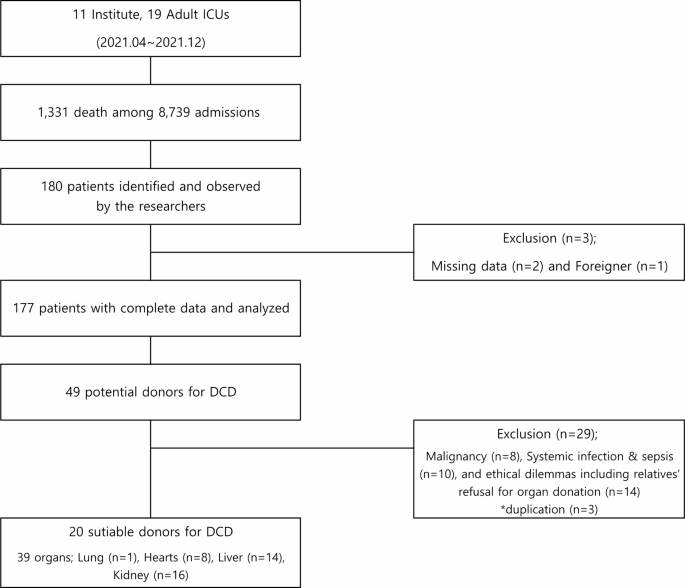
The primary objective of this study was to obtain basic epidemiological data on the proportion of patients with underlying and appropriate DCD status from Korean ICUs who died after discontinuing LST. Our study revealed that of the 177 patients who died after discontinuing LST, 20 (11.3%) were designated as suitable DCD donors. This is consistent with the results of previous studies.12,22. For example, data from the Potential Donor Audit, courtesy of the NHS Blood and Transplant Authority, shows that of the 3,825 potential cases of DCD between October 2009 and December 2010, 397 (10.4%) actually donated their organs. or have been classified as suitable for organ donation.twenty two. This dataset defines potential DCD donors, eligible or medically suitable DCD donors, and actual DCD donors according to guidelines published by the World Health Organization.27. In contrast to the study by Manara et al., our study was not a nationwide survey. However, we prospectively analyzed data from patients declared dead and screened potential DCD donors in a multicenter intensive care unit. According to medical and legal standards, all participants died after withholding or discontinuing LST. A single-center study in a French ICU found that of 76 patients classified as having foreseeable cardiovascular death on some form of life support, 32 (42.1%) could theoretically donate their organs. It was reported that the medical standards were met.12. In particular, Lesieur et al. They overestimated this rate because they included patients during LST rather than those who died after discontinuing LST. This indicates that the results of this study may more accurately reflect actual epidemiological data.
The key to successful organ transplantation is to shorten the warm ischemia time. In the French study, 32 patients out of a total of 79 patients were classified as eligible donors. However, only three patients (3.9%) died within 2 hours of discontinuing life support, a time frame thought to coincide with organ viability.12. In this study, we identified 20 medically suitable DCD donors according to established medical criteria. Of these, 14 patients died within 60 minutes of progression to systole after discontinuing life support, whereas 2 patients died between 60 and 120 minutes after discontinuing LST. The remaining patient experienced cardiac arrest approximately >2 hours after LST discontinuation, but this time frame was not compatible with organ donation. These results demonstrate that a standardized definition of medically qualified DCD donors, universal procedures for withholding/withdrawing LST, and clear standard criteria for cardiovascular death will reduce viable organ ischemia times. suggested that it is essential to
In contrast to the results of previous studies, the causes of death were significantly different in the present study. For example, the proportion of patients with hypoxic brain injury (14.3%) was lower in our study than that reported by Lesieur et al. (brain injury after cardiac arrest, 56%)12 and Manara et al. (hypoxic brain injury, 25%)twenty two. These differences may be due to differences in disease prevalence, medical practice, socio-culture, and ethical and legal frameworks for discontinuing LST.
This study also aimed to investigate the common practices and standards of death declaration in Korean ICUs. Of note, the majority of respondents declared the patient dead when observing a flat ECG signal. Based on previous studies, several European countries also use a flat ECG signal as a parameter for declaring DCD, and some countries also use invasive arterial blood pressure measurements or cardiac blood pressure measurements to declare death. We are requesting an additional ultrasound test. In particular, the UK Code of Practice suggests that cardiovascular death should only be declared after confirming the absence of a palpable pulse and audible heart sounds, which is defined by the presence of a flat ECG signal, the absence of a pulse. can be supplemented by Waves on invasive arterial blood pressure monitoring or lack of heart contractions seen on echocardiography28.
Most physicians (87.5%) in this study reported declaring cardiac death immediately or within 5 minutes after the ECG signal flattened. Furthermore, only 59.2% of respondents agreed that “5 minutes of no-touch'' time is sufficient to declare cardiovascular death. Nevertheless, among the physicians who opposed the 5-minute no-touch policy (66.1%), many believed that the 5-minute duration was too long. Meanwhile, 86.2% of physicians believed that cardiac death could be declared within 5 minutes. Remarkably, 13 out of 18 European countries have accepted a “5 minute no-touch” period as a national guideline or expert opinion.twenty three.
In Europe, where DCD is widely accepted, several countries have enacted legally binding national laws or non-legally binding national guidelines.twenty three. In this survey, 72.4% of respondents agreed that there is a need for legislation to define cardiovascular death and DCD.
To our knowledge, this is the first multicenter prospective study to evaluate DCD in South Korea and provide basic epidemiological evidence in this context. A total of 11 medical centers where organ transplant surgeries are performed participated in the study. In particular, adult patients who met modified Maastricht classification category III and were considered medically futile by a healthcare professional were considered. Additionally, this study adheres to common and precise medical eligibility criteria for organ transplantation, thereby ensuring accurate classification of DCD donors.
Our study also has some limitations. Because this was a multicenter study, death declarations were not consistently made by a single physician, especially at night. Additionally, not all ICU deaths were tested. We were not able to collect and monitor all patients who died after LST discontinuation in the ICU because all candidates were not immediately notified by the investigators. We only had access to the medical records of 180 decedents who were classified in category III of the Maastricht donation classification after circulatory death. Therefore, the number of patients who died or underwent DCD after LST discontinuation may be even higher.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish