
participants
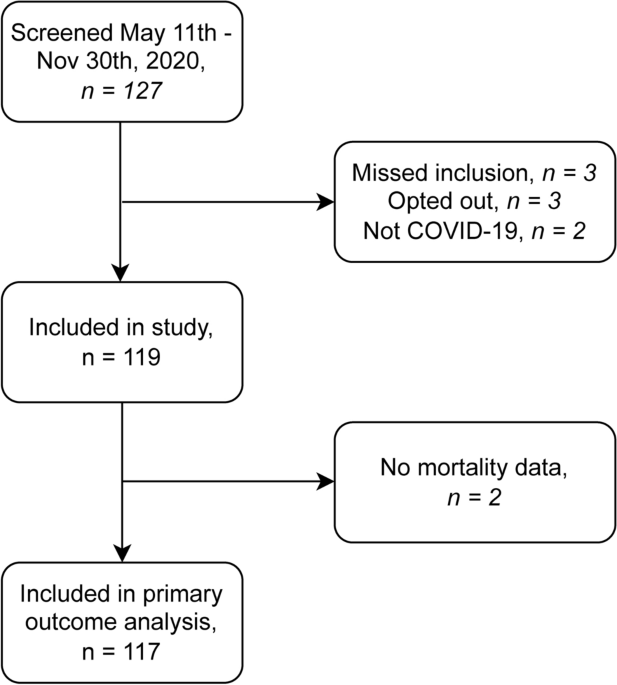
During the study period, 127 patients were screened for eligibility. The two patients tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) but were admitted to the hospital for other reasons. Three patients declined to participate, and three patients were initially excluded but were later deemed to meet the inclusion criteria and were therefore characterized as excluded inclusions. 119 patients were included and blood samples were collected. See illustration. 1. Of the included patients, 2 patients (1.7%) had missing mortality data in the population registry and were excluded from the primary outcome analysis, but had data on RRT.
Demographic/descriptive data
Baseline characteristics are shown in the table. 1. The overall 90-day mortality rate was 29% (34/117). Nonsurvivors were older, with a median age of 71.0 years. [66.3–80.5] vs. 62.0 years old [52.5–68.0] Among the survivors (p < 0.001). Approximately 75% of patients were male, and there was no difference between survivors and non-survivors. SAPS3 scores were higher in non-survivors (62.5 [53.0–71.0] vs. 51.0 [44.5–59.0], p<0.001). Nonsurvivors had higher CCI and higher incidence of chronic obstructive pulmonary disease (COPD, 35.3% vs. 15.7%). p = 0.035) and malignancy (17.6% vs. 3.6%; p = 0.028). There was no difference in the proportion active (3.6% vs. 2.9%; p = 1.0) before (49.4% vs. 61.8%; p = 0.3) smokers among survivors and non-survivors. Nonsurvivors were also slightly frail, with a Clinical Frailty Scale (CFS) score of 3.5. [2.6–4.8] vs 3.0 [2.0–3.0] (p = 0.002). Almost all patients met criteria for ARDS. A total of 18 patients required RRT in the ICU, with no difference between survivors and non-survivors. Of the deaths, 25 (94.1%) died before discharge and 2 (5.9%) died after discharge. In total, 22/119 (18.4%) developed or developed AKI upon ICU admission or within the first day. Median time to diagnosis of AKI was 1 day [0–1]. There was no difference in the incidence of AKI between survivors and non-survivors (19.3% vs. 17.6%; p = 1.0). The relative change in bio-ADM, expressed as mean (SD) percentage change, differed between survivors and non-survivors. In survivors, bio-ADM decreased by -4.1% (11.8) by day 2 of admission, by -9.1% (12.7) by day 7 of admission, and – from day 2 to day 7 of admission. Decreased by 6.9% (10.5). This is in contrast to non-survivors. In survivors, bio-ADM increased by 1.8% (11.0; p = 0.023) to day 2 of admission, 1.12% (13.2; p = 0.004), 3.2% (10.7, p<0.001) Days 2 to 7. In patients who did not require RRT, the mean (SD) change in bio-ADM was from admission to day 2 - 2.5% (11.36) and from admission to day 2 - 8.1% (11.7). This differed from patients who required RRT, where the mean (SD) change in bio-ADM was -0.6% (14.3, 10.8). p = 0.58) to day 2 of admission, 1.9% (18.3; p = 0.014), 3.5% (11.6, p = 0.015) from day 2 to day 7.
Bio ADM and mortality
Higher median bio-ADM was seen both at admission and in non-survivors (69.9 pg/L) [46.4–102.2 pg/L] vs. 51.4 pg/L [31.9–77.8 pg/L], p = 0.008), day 2 (69.9 pg/mL [44.3–108.1 pg/L] vs. 45.9 pg/mL [29.1–66.5 pg/L], p = 0.006) and day 7 (57.9 pg/mL) [39.6–91.7 pg/L] vs. 36.4 pg/mL [23.8–52.3 pg/L], p = 0.009). The percentages of missing bio-ADM values were 4.2%, 16.8%, and 38.7%, respectively. See illustration. 2.

Bio-ADM in survivors and non-survivors of severe coronavirus disease (COVID-19). Bio-ADM: Circulating bioactive adrenomedullin. ICU: intensive care unit. *: p-value < 0.05; **: p– value < 0.01.
Bio-ADM was associated with 90-day mortality in univariate Cox regression analysis at all three sampling times. The admission day sample had the lowest hazard ratio (HR 1.54, 95% CI 1.1 to 2.2; p = 0.02) compared to day 2 (HR 2.2, 95% CI 1.3 to 3.6; p = 0.003) or day 7 (HR 2.5, 95% CI 1.3 to 4.8; p = 0.007). All three models predicted 90-day mortality, with C-index for ICU admission of 0.66 (95% CI 0.57 to 0.75), 0.67 (95% CI 0.57 to 0.77), and 0.69 (95% CI 0.56 to 0.81). It was. 2nd and 7th day respectively, see table 2. Kaplan-Meier plots showed lowest survival in the third bio-ADM tertile at all three sample times. See illustration. 3.

Bio-ADM tertiles and survival in severe COVID-19 on days 2 and 7 of ICU admission. Bio-ADM: Circulating bioactive adrenomedullin. ICU: intensive care unit.
In multivariate Cox regression analysis adjusting for SAPS3, bio-ADM was not associated with mortality on admission (HR 1.48, 95% CI 0.91 to 2.43; p = 0.12), day 2 (HR 1.63, 95% CI 0.93 to 2.86; p = 0.087), or day 7 (HR 2.02, 95% CI 0.95 to 4.26; p = 0.066).
Using univariate Cox regression and observing changes in ADM values over time, the relative increase in bio-ADM from day 2 to day 7 was strongly associated with mortality (HR 1.10, 95 % CI 1.04 to 1.15, p < 0.001), and the relative increase from admission to day 7 was similar (HR 1.05, 95% CI 1.01 to 1.08; p = 0.0049) on hospital day 2 (HR 1.04, 95% CI 1.01 to 1.07; p = 0.020). The C-index was 0.74 (95% CI 0.62 to 0.85) for the relative change between days 2 and 7 and 0.70 (95% CI 0.58 to 0.81) for the relative change between the day of admission and day 7. , and 0.63 (95% CI 0.53 to 0.72). ) Regarding relative changes between admission and day 2.
The association between dynamic change and mortality remained even when SAPS3 was adjusted for change from day 2 to day 7 with multivariate Cox regression (HR 1.09, 95% CI 1.04 to 1.15; p < 0.001) and change from admission to day 7 (HR 1.04, 95% CI 1.01 to 1.07; p = 0.017), but not changes from day 2 of admission (HR 1.03, 95% CI 0.99 to 1.06; p = 0.11). The model also yielded a change in C index of 0.82 (95% CI 0.72 to 0.92) from day 2 to day 7 and 0.78 (95% CI 0.68 to 0.88) for change from admission to day 7. Predicted mortality.
Bio-ADM and ARDS severity
Bio-ADM on admission, day 2, or day 7 was not associated with severe ARDS (P/F ratio < 13) up to 7 days after sampling.
Bio ADM and RRT
Patients who required RRT during their ICU stay had a significantly higher median bio-ADM at ICU admission, 88.2 pg/L. [64.8–141.4 pg/mL] vs. 50.3 pg/mL [33.0–77.2 pg/L], p < 0.001), day 2 (94.4 pg/L) [71.5–160.4 pg/mL] vs. 46.4 pg/L [29.7–66.5 pg/mL], p < 0.001), day 7 (119.7 pg/mL) [67.3–146.7 pg/mL] vs. 35.7 pg/L [24.1–49.6 pg/mL], p < 0.001). Median bio-ADM increased over time (in consecutive samples) in the RRT group, whereas bio-ADM decreased over time in the non-RRT group.
Univariate Cox regression analysis showed that bio-ADM at ICU admission (HR 2.78, 95% CI 1.75 to 4.41; p < 0.001), day 2 (HR 5.28, 95% CI 2.49 to 11.16; p < 0.001), day 7 (HR 20.93 95% CI 4.95 to 88.63; p < 0.001) was associated with the need for RRT. Additionally, all bio-ADM samples predicted the need for RRT with C-indexes of 0.77 (95%CI 0.66 to 0.88), 0.84 (95%CI 0.75 to 0.92), and 0.89 (95%CI 0.81 to 0.97) It was. Samples from admission, day 2, and day 7, respectively, see table 3. In the Kaplan-Meier plot, the need for RRT increased with increasing bio-ADM tertile. See illustration. 4.

Bio-ADM tertiles and RRT-free survival on days 2 and 7 of ICU admission. Bio-ADM: Circulating bioactive adrenomedullin. RRT: Renal replacement therapy. ICU: intensive care unit.
In multivariate Cox regression adjusting for creatinine sampled at the same time as bio-ADM, bio-ADM remained associated with the need for RRT. HR at admission 2.43 (95%CI 1.26 to 4.69; p = 0.0082), HR on day 2 3.18 (95%CI 1.21–8.36, p = 0.019), HR on day 7 6.54 (95%CI 1.33 to 32.25, p = 0.021). The model also predicted the need for RRT, with C-indexes on hospital day 2 of 0.81 (95% CI 0.71 to 0.91), 0.91 (95% CI 0.87 to 0.96), and 0.94 (95% CI 0.90 to 0.98). 7th day each.
Univariate Cox regression of relative change in bio-ADM between sample and RRT showed an association between relative change in bio-ADM from day 7 of admission to need for RRT (HR 1.08, 95%CI 1.03 to 1.13, p = 0.0011), and the C index is 0.66 (0.46 to 0.86). There was no association with relative change from day 2 of admission (HR 1.02, 95% CI 0.98 to 1.07; p = 0.3) or change from day 2 to day 7 (HR 1.06, 95% CI 0.99 to 1.14); p = 0.084). In multivariate Cox regression adjusting for creatinine taken on the same day, relative change in bio-ADM from admission to day 7 was associated with RRT (HR 1.08, 95% CI 1.03 to 1.13; p = 0.0011), C-index 0.89 (95% CI 0.78 to 0.99). Relative change between day 2 and admission (HR 1.04, 95% CI 1.00 to 1.09; p = 0.075) and between days 7 and 2 (HR 1.03, 95% CI 0.98 to 1.09; p = 0.2), was not associated with RRT when adjusting for creatinine.
Bio ADM and AKI
Logistic regression was used to analyze the presence or development of AKI on admission and day 2 of Bio-ADM and ICU admission, with Bio-ADM on both admissions (odds ratio) [OR] 3.37, 95% CI 1.70–7.63, p < 0.001) and day 2 bio-ADM (OR 2.92, 95% CI 1.34 to 6.82; p = 0.009) was associated with AKI in univariate analysis. Multivariate logistic regression adjusted for SOFA score showed that both admissions Bio-ADM (OR 2.84, 95% CI 1.43 to 6.35; p = 0.005) and day 2 bio-ADM (OR 2.87, 95% CI 1.26–7.05, p = 0.01) was associated with AKI.
Bio ADM and IMV and Hospital LOS
Patients who required invasive mechanical ventilation (IMV) had higher median bio-ADM on day 2 (57.3 pg/mL) [41.5–88.3 pg/mL] vs. 34.9 [25.5–61.8 pg/mL], p = 0.003) and day 7 (49.4 pg/mL) [31.5–85.5 pg/mL] vs. 34.4 pg/mL [21.3–47.8 pg/mL], p = 0.004), than those who did not. Median bio-ADM values at ICU admission were not different between those who required IMV and those who did not (61.0 pg/mL) [37.8–83.3 pg/mL] vs. 45.5 pg/mL [31.5–84.6 pg/mL], p = 0.164). Linear regression analysis showed no association between Bio-ADM and mechanical ventilation duration on day 2 or 7 of ICU admission. Similarly, in linear regression analysis, there was no association between Bio-ADM at ICU admission or day 2 and hospital LOS. However, there was a weak association between bio-ADM and hospital LOS at day 7 (r2 = 0.06, p = 0.037).
bias
Patients with missing bio-ADM samples had similar demographics and comorbidities as patients without missing bio-ADM values. Patients with missing values had shorter IMV duration, shorter ICU LOS, and shorter hospital LOS. There was no difference in 90-day mortality (25% vs. 12.1%; p = 0.21). Of the total 357 samples, 71 (19.9%) were missing for various reasons. 15 (4.2%) due to patient death, 11 (3.1%) due to discharge from ICU, 2 (0.6%) due to transfer from participating ICU, 1 (0.3%) due to transfer from participating ICU %) due to patient withdrawal Further sampling revealed that 34 (9.5%) samples were lost or mishandled, and 8 (2.2%) samples were missing for unknown reasons. See table 4. No correlation was found between the time from collection to freezing and bioADM values (correlation coefficient R = 0.14, p = 0.068).
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish