
CKD is a common long-term complication after LT. Previous studies have shown that the incidence of CKD after LT varies widely.2,3,Four,Five,6,7,8,9,TenThis is mainly due to differences in the definition of CKD and follow-up period after LT. In a single-center retrospective study, Schmitz et al.3 We showed that 11.7% of liver recipients developed CKD, defined as serum creatinine ≤1.8 mg/dL ≤2 weeks, within 12 months. When follow-up reached 53.2 months, Fabrizi et al.8 We demonstrated that 28% of liver recipients developed CKD based on the definition of eGFR ≤60 mL/min/1.73 m.2Within 3 months. Using strict criteria according to KDIGO 2012 showed that the incidence of CKD after LT was 16.9% during a median follow-up period of 22.73 months. This was consistent with previous studies.
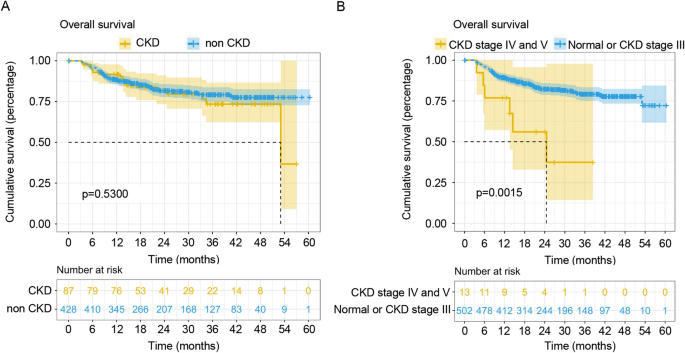
The relationship between CKD and poor prognosis after LT remains highly controversial. It has been reported that the onset of CKD is not associated with decreased survival11,22. This study also found that her CKD after LT did not reduce patient survival. However, both ours and previous studies showed a severe type (GFR < 30 mL/min/1.73 m) as the onset of CKD.2 or patients requiring renal replacement therapy) were significantly associated with increased mortality after LT2,23. LaMattina et al.Ten We retrospectively analyzed 1151 deceased adult LTs and found that 3%, 7%, and 18% of recipients developed ESRD at 5, 10, and 20 years, with an increase in severe CKD with extended follow-up. suggested an increase in the incidence of Therefore, early identification of CKD and early intervention in collaboration with nephrologists are highly necessary.
In this study, we established a new nomogram model to accurately predict CKD after LT. Before LT, we found it difficult to predict the occurrence of CKD after LT, as the AUC of preoperative parameters in model 1 was relatively low. In contrast, integrating postoperative parameters dramatically improved the predictive ability of the model. Independent risk factors for CKD after LT were older age of the recipient, prolonged anhepatic phase, low eGFR at 30 days after LT, and high TG level at 30 days after LT.
It is well known that older age is a risk factor for progressive renal dysfunction after LT2,9. Here, we found that for every year that age increases, the risk of CKD increases by 3%, confirming the above association. Older liver recipients generally have a higher risk of pre-existing renal dysfunction, metabolic disorders, hypertension, diabetes, and cardiovascular disease, making them more susceptible to CKD after LT.2, 24, 25. Considering the decreased clearance of immunosuppressants in the elderly, they are likely to be affected by immunosuppressant-induced nephrotoxicity, resulting in accelerated development of CKD after LT.24,26.
During LT, the inferior vena cava was partially blocked, and the portal vein and hepatic artery were completely blocked, which strongly influenced the hemodynamic changes of the recipient. Furthermore, a decrease in GFR and an increase in markers of renal damage (e.g., β2-microglobulin, N-acetyl-β D-glucosaminidase, syndecan-1) are observed during the anhepatic phase, which may lead to CKD after LT.27,28. Furthermore, prolonged anhepatic period increases the risk of graft dysfunction and metabolic disorders, mainly due to the accumulation of cytokines (such as interleukin-6), metabolites, and other toxic substances, which ultimately impair renal function. may worsen and reduce patient survival.29.
Previous studies have shown that high levels of TG are significantly associated with low eGFR in liver recipients.30. Our current study also found that TG levels at 30 days after LT are an independent risk factor for CKD, suggesting a potential role of hyperlipidemia in CKD development. I did. In CKD patients, changes in lipid profile include increases in low-density lipoprotein cholesterol and very-low-density lipoprotein cholesterol and decreases in high-density lipoprotein cholesterol.31,32,33. Such changes can increase lipid content (e.g., total cholesterol, TG), which can accumulate in the kidney and cause lipid nephrotoxicity.34.Considering the close correlation between hyperlipidemia and CKD, it is necessary to modulate lipid metabolism in recipients at high risk of CKD after LT.35. A series of clinical trials has shown that statins, with or without ezetimibe, can prevent and treat CKD.36,37,38,39,40,41. Furthermore, our previous study also demonstrated that proper control of blood glucose and lipid levels during the perioperative period of LT can reduce the incidence of chronic diseases after LT, such as metabolic disorders and CKD.42,43,44,45eGFR is commonly used as an indicator of CKD because its detection is accurate and convenient. Our study shows that low eGFR levels at 30 days post-LT are an independent risk factor for his CKD after LT, and early post-LT renal dysfunction contributes to the development of CKD. suggests that it is possible. In a retrospective cohort study, Sato et al.46 revealed that eGFR < 60 mL/min/1.73 m2 We proved our hypothesis that 1 month after LT was a predictor of CKD 2 years after LT. Blood loss during organ procurement and transplantation can cause intraoperative or postoperative renal damage, thereby affecting eGFR.46. These results highlight the importance of controlling eGFR early after transplantation. Additionally, efforts should be made to avoid significant intraoperative blood loss, use of nephrotoxic drugs, and acute kidney injury during LT.
Our study has several limitations. First, this was an observational study with a relatively limited number of cases and a short follow-up period. CKD is a slowly progressive disease, and the incidence increases with longer follow-up. Second, the nomogram model needs to be validated in a prospective study with well design. Third, given the small number of ESRD cases in our study, it is difficult to determine independent risk factors for ESRD and build a reliable model to identify those who develop ESRD and those who do not. requires larger, adequately powered studies with larger samples. Ultimately, the CLTR included more than 20,000 LTs between 2017 and 2020, but there was insufficient follow-up data to define his CKD after LT. was his only 118 case. Follow-up data entry and national database management are required.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish