
Study design and ethics
This retrospective cohort study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (approval number: 2209-100-1359). The IRB of Seoul National University Hospital waived the requirement for informed consent from participants because of the retrospective study design. We conducted this study in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).twenty threeand the Declaration of Helsinki.
Study population and data collection
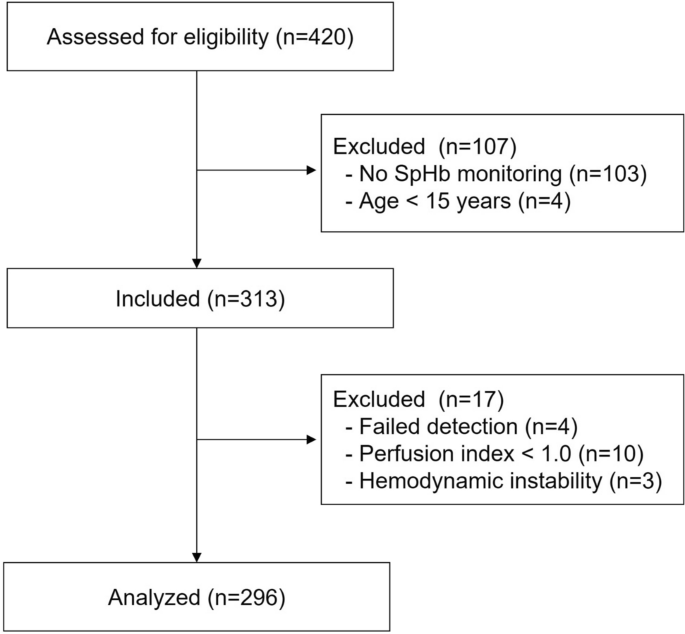
This study included patients who underwent liver transplantation at Seoul National University Hospital from November 2018 to March 2022. Patients without SpHb measurements and those under the age of 15 were excluded. Demographic data, including age, weight, estimated blood loss, and Model for End-Stage Liver Disease (MELD) score, were included.twenty fourLaboratory results for total hemoglobin and serum bilirubin were obtained from the electronic medical record. Estimated blood loss and transfusion volume of blood products were recorded at 5-minute intervals.
Time-matched SpHb and perfusion index values were obtained from a prospectively collected vital signs registry after approval by the Seoul National University Hospital IRB (H-1408-101-605) and registered in a publicly accessible clinical trial registry (ClinicalTrial.gov: NCT02914444).
Anesthesia Management
During the study period, the usual anesthesia management protocol for liver transplantation was performed. Anesthesia was induced using the mint model with an intravenous bolus of propofol (2.0 mg/kg) and an effect-site targeted controlled infusion of remifentanil in the concentration range of 3.0–4.0 ng/mL. Tracheal intubation was facilitated with rocuronium (1 mg/kg). After induction of anesthesia, a radial artery line was inserted using a 20G catheter to obtain blood samples. Anesthesia was maintained with sevoflurane 2 vol% to achieve a bispectral index value of 40–60. SpHb was continuously monitored using a Masimo adhesive sensor (R1 20L or R1 25L, rev E) connected to a Radical-7™ Pulse CO-Oximeter, software versions 7621 and 7801, placed on the fingernail bed. In addition, a light shield was applied to the fingertip to prevent optical interference.
Routine blood samples for complete blood counts (total hemoglobin) and liver function tests (serum total bilirubin) were collected at eight time points: immediately after induction of anesthesia, 1 hour after induction of anesthesia, 10 minutes after the start of the anhepatic phase, 5 minutes before, 5 minutes after, and 20 minutes after transplant liver reperfusion, 5 minutes after biliary reconstruction, and at the end of surgery. The exact time of each blood draw was recorded on the anesthesia chart. Total hemoglobin concentrations were analyzed using XE-2100 (Sysmex Corp, Kobe, Japan) and XN (Sysmex Corp) automated hematology systems. Serum total bilirubin levels were measured using a TBA 200FR (Toshiba Medical Systems, Ohtawara, Japan) chemistry analyzer.
Performance indicators
The primary outcome measure was the accuracy of SpHb with serum total bilirubin. Results were reported as bias, 95% LoA, and percentage error. Secondary outcome measures included the number and rate of potential overtransfusion and transfusion leakage based on SpHb.twenty five.
Subgroup analysis
We investigated several factors known to affect SpHb accuracy, specifically: (1) further investigating the subgroups of patients with total Hb levels <7.0 g/dL and >7.0 g/dL, the threshold that may trigger transfusion in critically ill patients;26(2) A subgroup that experienced massive bleeding (defined as bleeding ≥150 mL/min).27or patients who had received a blood transfusion within 5 minutes prior to the measurement. (3) Subgroups with a perfusion index of less than 1.4 and greater than 1.4, ensuring more conservative perfusion levels in critically ill patients.28(4) the ratio of conjugated bilirubin to serum total bilirubin, and (5) the intraoperative phase (including postinduction, dissection, anhepatic, and reperfusion phases).
Independent risk factors
Risk factor analysis for major treatment errors (grey or red zones in the error grid plot) was performed. Univariate analysis was followed by multivariate logistic regression analysis including factors such as total hemoglobin, perfusion index, serum total bilirubin, and conjugated bilirubin. Odds ratios and variance inflation factors (VIFs) with 95% CI for collinear diagnoses were calculated.
Statistical analysis
When calculating sample size, we made a conservative assumption that the probability of hyperbilirubinemia affecting SpHb was 0.1. G*power software version 3.1 was used.29A minimum sample size of 1367 was required to achieve a study power of 95% and an alpha error of 0.05. Patients were classified as normal (< 1.2 mg/dL)、軽度から中等度の高ビリルビン血症 (1.2–3.0 mg/dL)、重度の高ビリルビン血症 (> 3.0 mg/dL) were classified into three groups based on the serum total bilirubin criteria of the Child–Pugh scoring system (< 2.0 mg/dL、1 点、2.0–3.0 mg/dL、2 点、> 3.0 mg/dL, 3 points) was adopted.30Next, the accuracy of SpHb measurements was compared between groups.
To ensure accuracy of SpHb measurements, data recorded with a perfusion index < 1.0 or mean blood pressure < 60 mmHg were excluded from the final analysis. Data with missing values were also excluded. Descriptive statistics were applied to demographic and clinical data, and values were reported as mean ± SD or median (interquartile range). Variables were tested on a measurement rather than a patient basis. Agreement and accuracy of SpHb and total Hb concentrations in normal, mild-moderate, and severe hyperbilirubinemia groups were assessed by Bland–Altman analysis with multiple measurements per patient using MedCalc statistical software version 19.8.0 (MedCalc Software Ltd, Ostend, Belgium).31Repeated measures analysis of variance followed by post hoc analysis was performed to compare differences in SpHb and total Hb between groups.
Trend analysis was performed using four-quadrant plots to compare the differences between consecutive values of SpHb and total Hb to identify the direction and magnitude of change. A median exclusion zone was applied to exclude clinically insignificant changes <1.0 g/dL. Percentage agreement was calculated as the percentage of data points falling in the agreement quadrants (upper right and lower left). Reliable trend analysis ability was predefined as a percent agreement >90%.32,33.
An error grid analysis was performed to interpret the clinical impact of measurement error.34The error grid plot had three zones based on practice guidelines for perioperative blood management and clinical decision making.35,36,37Errors in the green zone had no further therapeutic impact because baseline and laboratory values had the same impact on decision making. On the other hand, errors in the grey zone could lead to significant therapeutic errors in transfusion management (Hb measurements of 10% or more) and errors in the red zone (Hb > 10 g/dL and SpHb < 7 g/dL, or Hb < 7 g/dL で SpHb > Errors within 10 g/dL (100–1000 g/dL) may pose a risk to patient safety despite the lack of benefit. The percentage of data in each zone was analyzed. < 7 g/dL で SpHb > We calculated the rate of missed transfusions when Hb was 7 g/dL and the rate of overtransfusions when Hb > 7 g/dL but SpHb < 7 g/dL.26Chi-square tests were performed to compare the number of major treatment errors, possible excessive transfusions, and possible missed transfusions.
of Naris 2 and ggplot2 Nonlinear regression analysis and Bland–Altman plots were performed using R packages, respectively. All statistical analyses were performed using R 3.2.0 statistical software (R Foundation for Statistical Computing, Vienna, Austria). P < 0.05 was considered significant.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish