
Research approval
This study was conducted in accordance with the tenets of the Declaration of Helsinki. The Institutional Review Board of Seoul National University Hospital approved the research proposal (approval number: H-2007-083-1141) and waived the requirement for written informed consent due to the retrospective study design. After approval, data were retrospectively collected from patients who underwent liver transplantation from January 2017 to October 2020. Patients younger than 15 years or those without recorded tacrolimus concentrations were excluded. We followed the recommendations in the article “STROCSS 2021: Strengthening the reporting of cohort, cross-sectional, and case-control studies in surgery.”37.
data collection
Twice-daily tacrolimus doses and whole blood tacrolimus concentrations measured by chemiluminescence immunoassay up to 14 days postoperatively were collected from the electronic medical records of Seoul National University Hospital for model training and internal validation. Ta. In addition, patient age, sex, height, weight, Model for End-Stage Liver Disease (MELD) score, donor type, indication for transplantation, and other immunosuppressive medications were recorded. Blood test results for alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin, international normalized ratio (INR), serum albumin, serum creatinine, and hematocrit were collected daily.38.
During the study period, patients received oral tacrolimus twice daily starting on day 1 after liver transplantation. Dose was determined empirically by the attending intensivist based on the patient's weight, liver and kidney function test results, and whole blood tacrolimus concentrations measured before taking the drug in the morning. Dose control and drug concentration monitoring were repeated until tacrolimus concentrations reached steady-state concentrations in the target range of 8 to 10 ng/mL.
model development
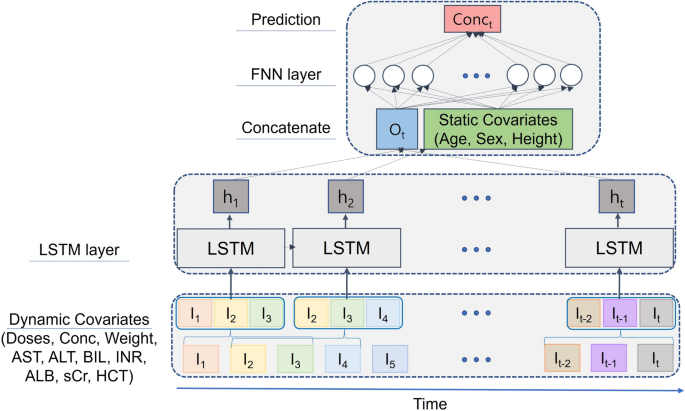
Oral tacrolimus administration history, measured whole blood tacrolimus concentrations, and time-dependent covariates (body weight, ALT, AST, total bilirubin, INR, serum albumin, serum creatinine, hematocrit) n number of days, and time-independent covariates (age, gender, height). The dataset included the following variables: n + 1 Consecutive days, first n Input is in a few days, output is in the last day. Additionally, missing values were imputed using multiple imputation. The tacrolimus concentration and dose before the first dose were replaced with zero.
A long short-term memory (LSTM) model was developed using input nodes for tacrolimus dose, measured tacrolimus concentration, and time-dependent covariates. The LSTM output was concatenated with time-independent covariates and input into a fully connected layer. These structures were inspired by the work of Lee et al.19.
Gradient-boosted regression tree (GBRT) and LR models were also developed for comparison. These models received the same inputs as the final LSTM models based on previous data. nday to day. GBRT hyperparameters such as number of estimators and maximum depth were also optimized using a similar method.
We employed a one-compartment PK model with first-order absorption developed for patients in the first 2 weeks after liver transplantation.39. PK parameters were adjusted based on posttransplant stage and serum albumin, AST, or hematocrit measurements. Apparent clearance (CL/F) was 8.93 and 11.0 L/h for AST ≥ 500 and < 500 U/L, respectively. The apparent volume (V/F) between days 0 and 3 after implantation was 328 L. After 4 days, the apparent clearance was set at 25.1 L/h if serum albumin < 2.5 g/dL or hematocrit < 28% and 17.1 L/h otherwise, and the apparent volume was 568 L.
Once the optimal combination of features and hyperparameters was identified, multiple random samplings were performed to evaluate the internal and external validation performance of the model.
Model training and validation was performed by the author's program written in Python (version 3.10.5) using the Keras library (version 2.10.0).
We compared the accuracy of the models with all combinations of the above variables for feature selection. Among the various combinations, the combination with the best performance in five-fold cross-validation and fewer variables was selected. We performed a grid search to determine the best combination of hyperparameters. The possible combinations of hyperparameters were 8, 16, 32, 64, 128, and 256 as the number of nodes in the LSTM. The number of nodes in the fully connected layer is 8, 16, 32, 64, and 128. The number of days you can enter is 2 to 7 days.
To increase the transparency of the model and reveal the influence of input features on the following tacrolimus concentrations, we apply the Shapley Additive exPlanations (SHAP) algorithm and perform feature-level explanation using SHAP version 0.39.0 in Python. further visualized.40. Briefly, SHAP summary plots were used to demonstrate the strength and direction of the association between traits and tacrolimus concentrations.
Internal verification
Multiple random sample validations were conducted. The sample of the derivation cohort was divided into training set (80%) and test set (20%) using 10 random seeds. We then repeated the training of the model using a similar method and estimated the average performance and 95% confidence interval.41. Prediction performance was evaluated based on root mean square error (RMSE), median absolute error (MAE), median error of performance (MDPE), and median absolute error of performance (MDAPE). Agreement between predicted and measured tacrolimus concentrations was assessed for each model.
external verification
For external validation, this study analyzed data from the eICU-CRD dataset of over 200,000 intensive care unit admissions in 208 U.S. hospitals between 2014 and 2015.twenty one. The “ward stay ID'' of a patient whose admission diagnosis was “liver transplant'' was extracted from the “hospitalization dx'' table. Patients younger than 15 years were excluded. Whole blood tacrolimus concentrations, ALT, AST, total bilirubin, INR, serum albumin, serum creatinine, and hematocrit measurements (labeled “Test Results Offset”) were queried from the “Tests” table. The tacrolimus dose was obtained from the 'Drugs' table and adjusted with the laboratory results based on 'Drug Start Offset', 'Drug Stop Offset', and 'Laboratory Results Offset'. Patients were excluded if the route of drug administration was sublingual or intravenous rather than oral. Data regarding age, gender, height, and weight were obtained from the “Patients” table. To ensure consistency with the training dataset, data with missing drug doses or concentrations were excluded. The LSTM, GBRT, and LR models predicted tacrolimus concentrations in this dataset, confirming the external validity of the model performance.
Recommended dose
The model suggested tacrolimus doses by first predicting tacrolimus concentrations for all hypothetical doses between the minimum dose (0.5 mg) and the maximum dose (20 mg). The dose of tacrolimus predicted to achieve the target concentration range (8–10 ng/mL) was then identified as the recommended dose. A 3 × 3 contingency table was created by aligning the administered doses against the recommended doses and the actual measured concentrations within the therapeutic range. Subsequently, these frequencies were statistically examined using the chi-square test.
Additionally, we evaluated whether dose adjustments to the proposed tacrolimus dose were associated with accelerated ICU discharge. We compared the length of ICU stay in patients who received tacrolimus within and outside the recommended range.
clinical outcome
We investigated whether high intrapatient variability, defined as tacrolimus concentrations outside the target range or the standard deviation of tacrolimus concentrations greater than 2 ng/ml, significantly impacts prognosis during the first 14 days after transplantation. I investigated.42. Clinical outcomes evaluated included transplant rejection, renal failure, and CMV infection. Transplant rejection was assessed by the transplant surgeon based on laboratory findings, biopsy results, and imaging studies43. Acute renal failure was defined as an increase in serum creatinine of 0.3 mg/dL or more within 48 hours or 1.5 to 1.9 times baseline in the previous 7 days.44. CMV infection was diagnosed using PCR assay45. Chi-square tests were used to analyze the association between tacrolimus concentrations and early posttransplant clinical outcomes.
Sensitivity analysis
A sensitivity analysis was performed to confirm the robustness of the LSTM model. Specifically, we trained the model without including drug concentration results and evaluated its performance.
statistical analysis
Due to the unique nature of a retrospective study, no formal sample size calculations were performed. Instead, this study used data available from a tertiary hospital and a large open dataset to develop and test a predictive model. Patient demographics and tacrolimus dose and concentration are described as mean (± standard deviation) or median (interquartile range) depending on the results of the Shapiro-Wilk test, and categorical variables are expressed as numbers (percentage). will be done. Continuous variables such as tacrolimus dose and concentration, age, weight, height, AST, ALT, total bilirubin, INR, serum albumin, serum creatinine, and hematocrit were compared using Student's analysis. t – test or Mann-Whitney U test. Categorical variables such as patient gender were compared using Pearson's chi-square test.
Model performance was evaluated using internal testing and external validation datasets. RMSE, MAE, MDPE, and MDAPE were compared using analysis of variance and then ex post factoT-test with Bonferroni correction. Based on previous studies, MDPE <20% or MDAPE <30% was considered clinically acceptable.twenty two,twenty three,twenty four.
Statistical analyzes were performed using Python and IBM SPSS for Windows version 21 (IBM, Armonk, NY, USA), and significant differences were considered.P< 0.05. The codes used for the analysis are attached in Supplementary Table S4.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish