
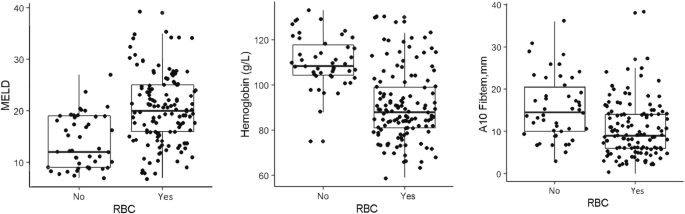
Factors associated with RBC requirements during and after 24 hours of LT in this study are consistent with previous studies5,10,11,12,13,14,15had high MELD scores and low baseline hemoglobin concentrations, indicated by a median hemoglobin concentration of 88 g/L in our cohort. These two factors clearly influence blood transfusion. Changes in hemostasis and coagulation laboratory parameters, including thromboelastometry values, were also associated with the need for RBC transfusion. However, after adjusting for MELD score and hemoglobin concentration, baseline PT/INR, fibrinogen concentration, platelet count, and Ex stem Values did not predict the need for blood transfusion. High baseline A10Fibtem Values supported no blood transfusions.
In our study, the presence of preoperative ascites was associated with higher transfusion requirements. Bleeding during LT is associated with portal hypertension, surgical difficulty, and hemostatic failure. In one large series, preoperative hepatic venous pressure gradient was associated with intraoperative bleeding, but hemoglobin concentration remained the main factor associated with red blood cell requirement.16 Nevertheless, portal hypertension has been reported to cause clinically significant ascites, which can lead to systemic hyperfibrinolysis.17. A10F was the only baseline factor other than hemoglobin concentration that favored non-transfusionibtem. However, if you raise A10F,ibtem In our trials, setting the target at 11 mm did not provide any clinical benefit.6.
Donor type was not associated with increased need for red blood cell transfusions or favoring non-transfusion. This is not surprising given that normothermic and hypothermic oxygenated perfusion devices currently improve post-purchase graft survival.18,19,20 Surgical times are longer, CIT is associated with higher red blood cell requirements, and the influence of a difficult surgical field has been identified.21,22.
One study found that machine learning was able to predict which patients were at risk of bleeding based on a number of preoperative and intraoperative variables.twenty threethe authors were unable to suggest any measures to reduce red blood cell requirements. In contrast, we used a regression model that generated separate predictions for expected packed red blood cell count and likelihood of non-transfusion, allowing factors that could be modified to potentially improve transfusion outcomes. I recognized it. The clinical urgency of doing so is illustrated by the fact that 24% of transfused patients received 6 or more units of packed red blood cells.
We observed a decrease in plasma fibrinogen concentrations in both groups during LT, even though baseline plasma fibrinogen concentrations were not associated with red blood cell requirement after adjusting for cofactors. The decrease in plasma levels of fibrinogen during reperfusion of the liver graft relative to the value of the hepatic phase was also higher in the transfused group than in the non-transfused group (median decrease, -0.44 vs -0.22 g/l). Regardless, 77% of patients in the transfusion group received concentrated fibrinogen, compared with 39% in the nontransfusion group. This fact was more pronounced in patients who presented with PRS.
After graft reperfusion, several events occur simultaneously. restoration of normal splanchnic circulation, addition of irrigated liver perfusate, and release of substances from the new graft.twenty four. PRS is caused by liver graft and recipient risk factors, and refrigerated perfusate in liver grafts causes known effects such as hypothermia, hyperkalemia, and hypervolemia, and these phenomena are common in large grafts. It becomes noticeable. The combination of these events can result in extensive surgical bleeding and severe hemodynamic compromise. In our series, PRS was associated with a bolus injection of tranexamic acid. 47.56% of PRS patients received tranexamic acid during reperfusion. Reasons that could explain this scenario include some degree of hyperfibrinolysis associated with hypotension.25,26specifically, continuous oozing bleeding or long clotting times (more than 300 seconds on A10F)ibtem extreme case of our cohort), MCF Ex stem<15 mm.
Some modifiable intraoperative risk factors were associated with greater transfusion requirements, such as the presence of PRS and fibrinolysis. Identification of these factors suggests that devising protocols before reperfusion of liver grafts may improve outcomes. Therefore, “timing” is important, but performing this action before reperfusion of the liver graft has not been considered. In this protocol, we recommend a bolus injection of 500 mg tranexamic acid to prevent PRS with vasopressor support and prevent possible fibrinolysis. Although such a strategy is feasible, it will require support from data from randomized clinical trials.
For clinically compensated candidates whose pre-LT pathology has not changed according to standard measurements and MELD status, only hemoglobin optimization can clearly impact RBC requirements. Anemia, which occurs in approximately 25% of patients with cirrhosis, is multifactorial and involves iron and vitamin B deficiencies, hypersplenism, hemolysis, gastrointestinal bleeding, bone marrow deficiency, and hepatitis C virus treatment.27,28. Anemia was associated with bleeding and major postoperative complications, and 1-year mortality in two retrospective series5,29. In another series of patients with cirrhosis, oral iron correction improved hemoglobin levels.30. In our cohort, the median value in the highest quartile of patients who did not receive RBCs was 118 g/L. Despite the clinical difficulty of optimization in patients with liver disease, this value suggests targets for testable preoperative optimization strategies.31. Based on the studies we reviewed and the findings we report here, we believe that hemoglobin optimization merits further consideration as a modifiable preoperative factor using intravenous iron for waitlist candidates. I'm thinking.
The main limitations of this study were related to the study's exclusion criteria. Patients were excluded that would have clearly affected RBC requirements. The analysis may have been modified by excluding 93 patients with hemoglobin concentrations ≥130 g/L and for whom transfusion was not anticipated. Another limitation is related to the small number of massively transfused patients compared with older retrospective outcome studies.10,12. In our series, only 32 patients (18.2%) required six or more RBCs. Therefore, the extent of the influence of these patients on major complications in the group of transfused patients is limited, especially when the incidence of major complications is downloaded, as happened in our study. Nevertheless, the patients in our series are comparable to those currently included in the waiting list of European registries.32. However, although this does not necessarily change the conclusions we can draw, our cohort was not previously assumed to be at risk and may have benefited from interventions to reduce transfusion requirements. We need to emphasize that we represent the patients. We believe that this finding supports the clinical value of our results. A strength of this study is the quality of patient recruitment and data collection, which was monitored by an independent committee and is available upon request.
We conclude that correction of anemia in LT candidates should be included in preoperative patient blood management protocols. We also propose a randomized clinical trial to test strategies to prevent PRS and fibrinolysis during graft reperfusion.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish