
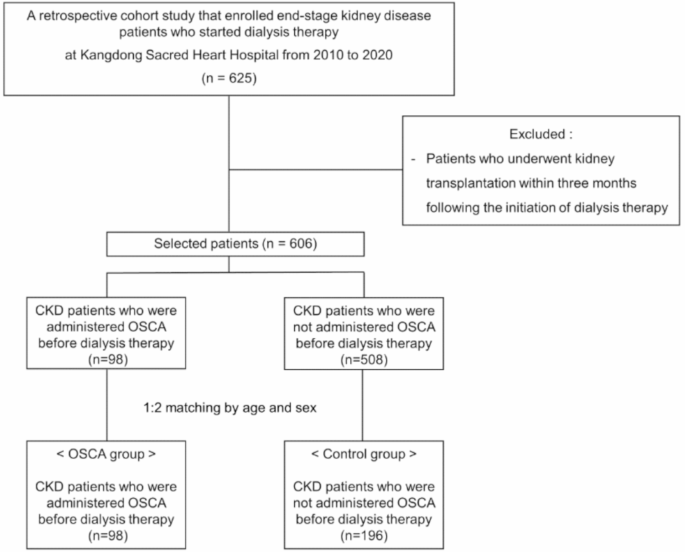
This retrospective cohort study evaluated the effects of Osca administration during predialysis CKD on cardiovascular outcomes after initiation of dialysis therapy. We analyzed 294 patients, including 98 people who received Osca before dialysis and 98 people, including 196 controls. Patients who experienced OSCA for more than 4 months had significantly fewer cardiovascular events than those with shorter postdialysis (patients who received OSCA for a shorter period (i.e., 2019).p= 0.032). The multivariate COX model revealed a reduced risk of cardiovascular events in the OSCA ≥4 month group compared to the control group (HR 0.39, 95% CI 0.18–0.84). Furthermore, patients in the OSCA ≥4 month group experienced significantly fewer combined results than patients in the control group (HR 0.46, 95% CI 0.24–0.90). These findings indicate that long-term use of osca before the onset of dialysis can reduce cardiovascular events and post-dialysis deaths, suggesting a potential “heritage effect.”
China et al.twenty two We demonstrated that administration of osca prevents the development of left ventricular concentric changes in patients with predialysis CKD. Sato Eltwenty one. OSCA treatment reported to be independently associated with dialysis induction, mortality, cardiac events, and low risk of stroke.18 We reported the protective effect of Osca against major cardiovascular adverse events. However, these studies investigated the effects of OSCA on clinical outcomes in patients with predialysis CKD. In particular, another study evaluated the effect of Osca treatment on patient prognosis on hemodialysis. They reported that the 5-year survival rate was significantly higher in the Osca group, and the risk of death was 1.91 times higher in the non-Osca group.twenty three. This finding is similar to the results of the study.
Several hypotheses have been proposed regarding the pathophysiological mechanisms in which uremic toxins affect cardiovascular disease. Indoxyl sulfate and ADMA are known to play a pivotal role in the pathophysiology of these complicationstwenty four. Experimental studies have shown that indoxyl sulfate levels are increased after myocardial infarction, with increased numbers of renal injury biomarkers and oxidative stress markers in serum and renal tissue. However, osca administration has been found to reduce these markers, and indoxyl sulfate is associated with the pathophysiology of cardiac syndrome, suggesting that osca administration may alleviate renal and cardiac damage caused by these substances.twenty four,twenty five,26. The main role of ADMA is to reduce nitric oxide production, thereby adversely affecting blood pressure, vascular tone, platelet aggregation, leukocyte adhesion, and vascular smooth muscle cell proliferation, affecting the cardiovascular system.twenty four,27,28. As a result, ADMA promotes the progression of atherosclerosis and hypertension, affecting the development of cardiovascular disease. Furthermore, laboratory data show that ADMA inhibits osteoblast differentiation29suggests that ADMA may contribute to the development of mineral disorders in CKD. Our findings suggest that administration of osca not only slows the progression of CKD, but also has a “heritage effect” in reducing cardiovascular morbidity and post-dialysis mortality after mortality, primarily by reducing the detrimental effect of uremic toxins on the cardiotoxin system. This study highlights the potential of OSCA as a therapeutic measure to enhance clinical outcomes in patients with ESKD, and ensures further research to explore long-term benefits and mechanical insights.
This study revealed hemoglobin, serum proteins, serum albumin, and total serum CO.2 LDL levels were significantly higher in the OSCA group than in the control group. These findings suggest that osca administration may ameliorate the adverse effects of uremic toxins on erythroderma, nutritional status, and metabolic acidosis, and may promote cardiovascular outcomes and patient survival. Furthermore, the positive effects of Osca on lipid metabolism may contribute to the prevention of cardiovascular disease. Although not statistically significant, BUN levels were generally higher in the control group just before the onset of dialysis, suggesting better clinical compliance potential among patients in the OSCA group. These results indicate that OSCA may reduce the deleterious effects of uremic toxins on the cardiovascular system and suggest a lasting “heritage effect” that may affect cardiovascular health and mortality even after the onset of dialysis.
This study has several limitations. First, its retrospective cohort design and non-random allocation of Osca treatment introduces a potential selection bias. To alleviate this, patients were matched based on age and gender and multivariate analyses were performed, adjusted for various covariates. Comparing clinical characteristics, no differences were found between the two groups regarding the underlying causes of ESKD, height, weight, BMI, hypertension, and DM. Presence of CAD prior to dialysis, proteinuria, socioeconomic status, treatment compliance, and drug use such as ARB/ACEI, statins, and aspirin. However, other unmeasured confounders may affect the results of our study. Second, the single-center nature and relatively small sample size limit the generalizability of the findings. Given these limitations, our results should be interpreted with caution, particularly as the results of subgroup analyses increase the risk of type II errors. Future research should focus on implementing a Prili-power calculation to determine the appropriate sample size. We consider multicenter collaboration to increase sample sizes, pre-specify subgroup analyses, ensuring appropriate power for these analyses, while also highlighting the need for replicating findings in larger, more robust studies. Third, most laboratory data were measured at the onset of dialysis. This may vary depending on the nephrology clinician's policy regarding the initiation of dialysis.
In conclusion, patients who received long-term OSCA during the predialysis period for CKD had a lower incidence of cardiovascular events and death after initiation of dialysis therapy, suggesting a more likely “legacy effect” than patients who did not undergo OSCA. Our results suggest that osca administration in predialysis CKD patients may be considered not only to slow CKD progression, but also to improve the prognosis of ESKD patients after the onset of dialysis. A sufficient period of administration of Osca during the predialysis period is recommended to improve postdialysis prognosis.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish