
Several studies have been conducted on the influence of HLA compatibility on post-LT outcomes. Several previous studies showed that higher HLA compatibility was associated with a lower probability of acute rejection after LT, but the impact on overall graft survival remained controversial. .2,9. Donaldson et al.3demonstrated that HLA class I matching can influence graft survival by increasing the likelihood of acute rejection and the development of bile duct vanishing syndrome. However, by analyzing his OPTN database, Navarro et al.Ten showed that there was no clinically significant relationship between the degree of HLA matching and 5-year graft survival in LT. Recently, Bricogne et al.11 found that locus-specific HLA-A mismatch was associated with transplant failure and poor patient survival after LT by increasing hepatic artery thrombosis and sepsis.
Efforts are also being made to find a relationship between HLA compatibility and GVHD after LT. Several previous studies have highlighted the importance of D → R unidirectional HLA MM as a strong risk factor for GVHD.12, 13. However, because the prevalence of GVHD is so low, it has been very difficult to find research on this topic in the past few decades. A previous study published by Kim et al.14A retrospective single-center study showed that D→R unidirectional HLA MM at 3 loci significantly increased the incidence of GVHD after LT. However, our study was designed as a large multicenter study using prospectively updated data from the KOTRY registry. In this study, by comparing the D→R unidirectional HLA MM patient group with the D→R unidirectional HLA MM patient group, we found that there was a significant difference in the incidence of GVHD between these two groups. has become clear. Furthermore, for the D→R unidirectional HLA MM patient group, we further divided it based on the number of MM locus differences and analyzed the risks of GVHD, graft failure, and patient survival. This shows that this phenomenon is not limited to a single center and that similar results occur in other centers.
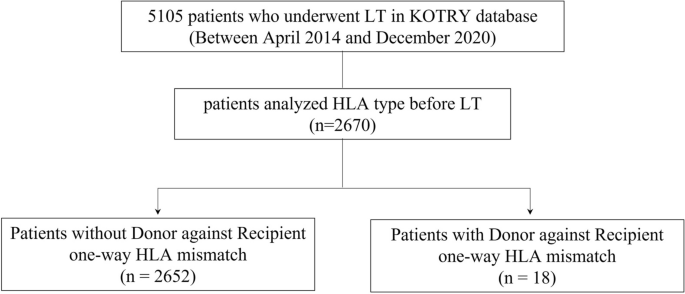
Because this study is based on KOTRY data, it is difficult to review the clinical course of each patient. Therefore, GVHD may be underdiagnosed in the study population. However, even considering the exclusion of some her GVHD patients due to underdiagnosis of GVHD, we found a much higher incidence in the D→R unidirectional HLA MM group. Approximately 0.4% (11 of 2670 patients) of the total study cohort in this study were reported to have GVHD after LT. A total of 22.2% of patients in the D→R unidirectional HLA MM group were reported to have GVHD, whereas only 0.3% of patients in the control group were reported to have GVHD. To more accurately analyze the relationship between GVHD and D→R unidirectional HLA MM, we analyzed her HLA type at each locus (HLA-A, -B, -DR) in all her GVHD patients after LT. was analyzed. Interestingly, 4 of 6 living donor LT cases with GVHD showed D→R unidirectional HLA MM, whereas no deceased donor LT cases with GVHD showed D→R unidirectional HLA MM. . In particular, D → R unidirectional HLA MM at the 3 locus occurs when an HLA homozygous donor and an HLA heterologous recipient share a haplotype, and this HLA type combination is typically transplanted between parent and child. Occurs when the Indeed, in the present study, all recipients who suffered from GVHD after living donor LT received liver transplants from their offspring, and D→R unidirectional HLA MM was seen in the majority, which suggests that GVHD after living donor 66.7% of affected recipients. L.T.
Previous studies have found that strict HLA type matching between donor and recipient, recipient age, and glucose intolerance are risk factors for GVHD after LT.4, 6, 8. However, in our study, D→R unidirectional HLA MM was the only significant independent risk factor for her GVHD after LT. In multivariate analysis, D→R unidirectional HLA MM at 3 loci and D→R unidirectional HLA MM at 1 or 2 loci appeared to be highly associated with GVHD with odd ratios of 163.3 and 91.85, respectively. . On the other hand, D→R unidirectional HLA MM is not associated with post-LT graft failure, and D→R unidirectional HLA MM at 1 or 2 loci is not a risk factor for patient mortality. There was found. Only 3-locus D→R unidirectional HLA MM was identified as the strongest risk factor for patient mortality. These findings indicate that D→R unidirectional HLA MM at the 3 loci is one of the strongest risk factors for GVHD, which can lead to devastating outcomes such as patient death. . Additionally, Kaplan-Meier survival curve analysis showed that only D→R unidirectional HLA MM at 3 loci, but not D→R unidirectional HLA MM at 1 or 2 loci, compared with patients with showed a significantly lower patient survival rate. Does not have D→R unidirectional HLA MM. There was no significant difference in death-censored graft survival between the D→R unidirectional HLA MM group and the control group. There was no statistically significant difference between the two groups regarding rejection-free survival. However, we observed that there was no incidence of rejection in the group of patients with D→R unidirectional HLA MM. From the recipient’s perspective in the setting of D→R unidirectional HLA MM, there is no mismatch with his HLA of the donor, meaning that donor-specific antibodies (DSA) are very unlikely to be present. . This can be seen as a finding confirming the results of previous studies suggesting that DSA may influence rejection after liver transplantation.15,16,17,18.
A limitation of this study is that it is a retrospective multicenter study using KOTRY data, so there is a lack of information about other types of HLA alleles such as HLA-C, -DQ, and -DP, and these HLA alleles is difficult to analyze. . Similarly, we were unable to use his more recent and more accurate PCR-based HLA typing data. Previous studies on hematopoietic stem cell transplantation have shown that antigenic mismatch at the HLA-C*14:02 locus can increase the risk of GVHD, and similar antigenic mismatch also affects liver transplant outcomes. It has been suggested that it may have negative effects.19. However, Hirata et al.20 reported that the effects of HLA-C, HLA-DQ, and HLA-DP on GVHD were less pronounced than HLA-A, HLA-B, and HLA-DR. In the future, the accumulation of additional data on high-resolution sequence-based HLA typing and epitope matching may enable further research and, in particular, to undertake more precise mismatch analysis that may impact liver transplantation outcomes. We expect that there will be. GVHD. It was also difficult to examine the specific clinical course of each case from the KOTRY data. Therefore, some cases may not be diagnosed as GVHD because the symptoms are nonspecific and a definitive diagnosis of GVHD is difficult. However, as a result of prospective multicenter data collection, HLA type, specifically 3-locus D → R unidirectional HLA MM, is a highly lethal prognostic factor for the occurrence of both GVHD and patient mortality. , which has strength in the generalizability of the findings. .
Although some studies have reported the risk of D→R unidirectional HLA MM at the 3 loci of GVHD, its importance has been less emphasized in the general field of LT as cases of living donor LT still exist. I’d guess not. D → R using unidirectional HLA MM. This may be due to the minimal reported data on this subject, as the odds are very low even in his LT setting for living donors. Until the LT community finds a solution to this devastating condition, the only solution is to avoid transplants with this high-risk donor-recipient combination.
In conclusion, among patients considering living donor LT, if the donor’s HLA type exhibits a homozygous pattern and shares HLA haplotypes with the recipient, D → R unidirectional HLA MM at the 3 loci probability is very high. GVHD. This can have fatal consequences and lead to death of the patient. Therefore, in such cases it is necessary to select an alternative donor or refrain from transplantation. However, in the case of deceased donor LT, although the possibility of developing D→R unidirectional HLA MM is extremely low, the possibility of GVHD occurring still exists, so for his GVHD occurring during deceased donor LT, Further research is needed.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish