
ethics statement
After signing the data agreement (November 11,187, 2021), we analyzed data from the Surveillance, Epidemiology, and End Results (SEER) database. Furthermore, our study was exempted from ethical review. This article does not contain any data obtained by the authors with human participants.
Study population
SEER*Stat version 8.4.0 was used to retrieve patient data from the SEER Research Plus Data, 17 Registry, November 2021 Sub (2000-2019) incidence database. This study included a total of 2,538 patients with ICC after curative surgery and 5,048 patients with HCC after LT. The following variables were used in the analysis: patient age, sex, race, marital status, American Joint Committee on Cancer (AJCC) stage, tumor size, tumor grade, surgical approach, radiation therapy (Y /N), chemotherapy (Y/N)), fibrosis score, survival months, and OS status.
statistical analysis
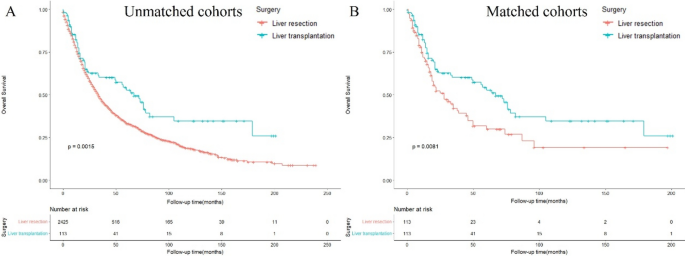
Baseline characteristics of ICC patients after LR and LT were compared using the Kruskal-Wallis test and χ.2 Tests performed on continuous and categorical variables, respectively. Propensity score methods were applied to control for possible effects of measured confounders. The propensity score is a multivariate logistic model that includes patient age, gender, race, marital status, AJCC stage, tumor size, tumor grade, radiation therapy (Y/N), chemotherapy (Y/N), and fibrosis score. Calculated using a regression model. A balanced cohort was created using a one-to-one nearest neighbor propensity score matching (PSM) method.16. Survival rates were estimated using Kaplan-Meier survival curves and compared using the log-rank test.
All statistical analyzes were performed using SPSS (version 24.0; SPSS, Chicago, IL, USA) and R software (version 4.1.2; http://www.r-project.org/). Statistical significance was set as follows. p≦0.05.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish