
As previously observed, our results suggest that, considered as a whole, the psychosocial status of LKD remains stable after donation3, 9, 30, 31. Few adverse psychosocial outcomes following donation were observed. However, subgroups of donors who need more information about the risks of surgery, or those who donated out of fear of losing the recipient/commitment to stop their suffering, may find that some aspects of HRQoL are Slightly worse. It appears that both variables are subject to change during the donor selection process.
Previous studies have reported that 10–31% of LKD believe that more information about donation should have been provided preoperatively.16,32. Perceptions of not having enough information before donation have been proposed as a determinant of donor dissatisfaction after donation, especially when the information received before donation and the donor’s actual experience differ significantly .33. Recognizing the need for further information about the surgery and its risks must be carefully considered to answer all questions of potential LKD and to ensure that they feel ready to donate. Furthermore, the need for more information may be due to insufficient information, but in some cases it may also be an expression of ambivalence toward donation. This clinical attitude, aimed at ensuring the legitimacy of the informed consent process, should also include disclosure of risks newly recognized in the literature.15.
We have already mentioned that the strongest motivation for donating LKD is the desire to improve and/or save the recipient’s life.34. However, LKD may not take into account some variables related to recipients’ post-donation behavior that are outside of their control, such as treatment noncompliance or excessive alcohol consumption. These post-donation issues can worsen the donation experience by causing disappointment and damaging the donor-recipient relationship.35. Furthermore, donations that are primarily motivated by a perceived need to save the recipient’s life may influence the decision-making process of LKD by speeding up the donation process.36. Similarly, a sense of obligation or primary responsibility for the recipient’s health, with aspects of pressure or coercion (e.g. by family), can undermine donor autonomy in decision-making and, in turn, impair postoperative psychosocial outcomes. There is. These scenarios may have made donors feel unready to donate. Both involve the rapid identification of common, urgent and unwarranted needs to save the recipient’s life, and the investigation and resolution of the recipient’s actual life risks (e.g. by discussing alternative interventions such as dialysis). ) may help ameliorate this risk factor. Additional research on LKD donation motivations is needed to replicate our factorial solution. We considered the motivation questionnaire to be an interesting tool that could be useful for future research.
Subjective socio-economic status reported a small but statistically significant improvement after donation. This improvement may be related to improved physical health in the recipient. For example, two-thirds of her recipients were on dialysis before transplantation. After transplantation, given that all donors are genetically or emotionally related, both recipient and donor will be freed from the out-of-pocket costs associated with dialysis treatment, and the recipient may be able to resume a full working life. There is a gender. It has a positive effect on the socio-economic status of donors. Although changes in employment status were not measured in our study, recent studies have shown that the proportion of recipients who returned to work 1 year after transplantation depends on the type of work.37. Additional research is needed to confirm the improvement in socio-economic status and define its determinants.
Comparing pre-donation and post-donation HRQoL showed statistical significance for the reduction in three scales of the SF-36. Two of them measure physical factors. physical role (how much physical health affects work and other daily activities) and physical pain (intensity of pain and its impact on activity). Last vitality indicates decreased energy and increased fatigue. Although this is usually associated with the mental component of HRQoL, it certainly affects the physical component as well. Vitality scores may remain slightly lower in the long term, and further investigation is required to define whether decreased vitality scores are a result of donation or a combination of multiple factors.30and whether it is the most affected component of HRQoL affected by donation.15. It is important to emphasize that these reductions are clinically meaningful only on the somatic pain scale, which is outside the normal range for the general population.
A higher proportion of donors with decreased HRQoL reported an increased risk of poor post-donor physical health (donor complaints or illness still present and postoperative recovery considered more difficult than expected). Ta).Donor experiences of physical complications and long recovery periods are associated with functional impairment and health status years after donation26. One year after donation, LKD will conduct more limited medical follow-up to quickly identify medical and psychosocial complications. Nevertheless, his LKD with decreased HRQoL felt anxious about their health, and the proportion was higher after donation.
Contrary to our expectations, we found no association between recipient medical characteristics (pre- and post-transplant) and donor psychosocial outcomes. Previous studies have shown that recipient outcomes can influence donor QoL and mental health. However, their results are contradictory, indicating negative effects of one or the other.11,29,36or no association between recipient medical comorbidities and donor psychosocial outcomes.26, 31, 38. High-risk recipients (e.g., hyperimmunized patients) or with perioperative complications (e.g., bleeding, hematoma, wound infection), or long-term complications (e.g., graft failure and recipient death) prior to donation Close monitoring of donors could lead to even more important monitoring. Insights into this field. Our recipient follow-up was limited to 1 year, and the incidence of graft failure and recipient death was correspondingly low. Longer follow-up of recipients and donors is needed to examine the actual impact of these variables on the psychosocial outcomes of LKD29.
Limitations
Data on surgical procedures (laparotomy vs. laparoscopic nephrectomy) were not included in the statistical analysis, so we do not know whether the inclusion of these variables would change the structure of the clusters.However, according to the available literature, differences in surgical technique do not seem to be significantly associated with his HRQoL outcomes39,40,41,42.
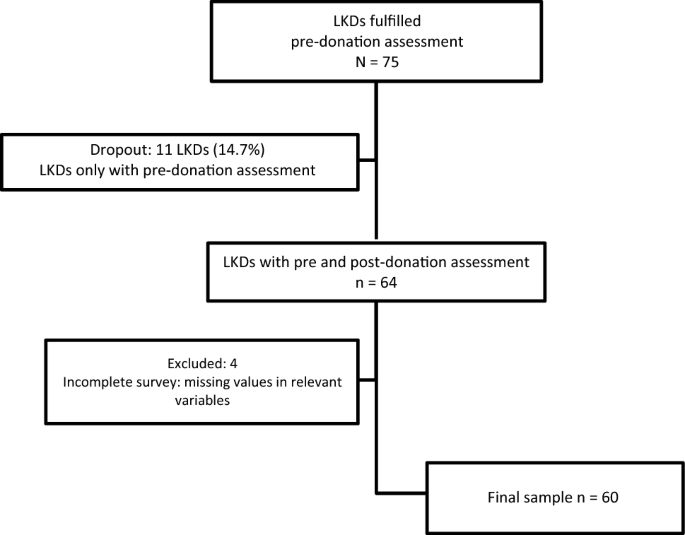
We cannot determine whether donors who only completed the pre-donation questionnaire (13.9%) avoided participating in the follow-up process due to dysfunctions of a psychosocial or physical nature. In our study, completers were characterized by lower levels of depression and higher scores on the Personality Extraversion Scale.Depression is associated with poor adherence to self-care plans and increased complications in patients with chronic illness43. Additionally, adaptive personality traits such as high extraversion (a tendency to have positive emotions and interpersonal relationships) were found to be the only personality traits significantly correlated with post-donation growth.44. Therefore, it may not be possible to discard a “self-selection” bias in a sample of donors who have more resilient characteristics and are more likely to respond to post-donation questionnaires. Therefore, these results should be considered with some caution.
The follow-up sample size did not allow for separate analyzes by transplant center. Center-specific practices may impair the generalizability of our results (e.g., center policies that select donors with comorbidities or national policies that restrict donors by type of donor-recipient relationship). regulations, etc.). Including other centers may increase the number of participants to help resolve this issue. Additionally, the limited sample size reduced statistical power, especially in multivariate analyses.
We used the general population, including subjects with chronic diseases, as reference data for the SF-36 T-score. As suggested by previous authors, comparisons with healthy populations may be desirable.11. However, in a selected healthy cohort, as some his LKD may have hypertension or metabolic disorders prior to donation, and healthy populations do not undergo surgical intervention comparable to kidney donation. Even if there is, it may not be appropriate.45.
To determine whether the changes observed in psychosocial domains in LKD also occurred in the absence of donation, and whether these changes are no different from those observed in the general population as normal fluctuations. No control group was included.13.
Our cluster 2 was characterized by a short elapsed time between donation and post-evaluation. This difference may be caused by variations in each participant’s responses to post-donation surveys, such as the amount of time elapsed between receipt of mail and time elapsed between receipt and completion of donation. It is well known that his HRQoL in LKD usually returns to baseline or remains slightly decreased over time.3, 30.
Kidney recipient variables were evaluated from a medical perspective only, and sociodemographic and psychosocial variables were not collected. Therefore, it is impossible to determine whether the recipient’s psychosocial status (pre-transplant and post-transplant) influenced the donor’s psychosocial outcome.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish