
Source of data
Study participants were identified from the Diagnostic Procedure Combination (DPC) Inpatient Database, a Japanese administrative claims database. This database includes more than 1,000 of his hospitals, including all 82 university hospitals, and covers more than half of all inpatient admissions in the country.16. The DPC database provides information on various aspects such as diagnosis at admission, comorbidities, and cause of death coded according to the International Classification of Diseases and Related Health Problems, 10th edition (ICD-10).17. It also includes patient information such as age, gender, body mass index (BMI), admission and discharge status, his ADLs at the time of admission and discharge, and comorbidity score known as the Charlson Comorbidity Index.18updated for risk adjustment19,20. This study was conducted in accordance with the ethical principles set forth in the 1964 Declaration of Helsinki and was approved by the Tokyo Medical and Dental University Ethics Committee (No. M2000-788). Due to the anonymity of the data, the Ethics Committee of Tokyo Medical and Dental University waived the requirement for informed consent.
In 2020, there were 338,256 pneumonia-related cases in the DPC database, either as the primary diagnosis during hospitalization, as the reason for hospitalization, or as the disease requiring the highest medical costs. Inclusion criteria for this study were patients aged 18 years or older, length of hospital stay longer than 24 hours, and primary diagnosis of hospitalization being either his COVID-19 or pneumonia (Figure 1). S1). COVID-19 pneumonia and non-COVID-19 pneumonia were recognized by ICD-10 codes. A number of patients including second or subsequent hospitalization, death within 24 hours of admission, BMI <15 or >50, incomplete information on BMI, ADL, type of admission (urgent or non-urgent), and patients with aspiration. Exclusion criteria were applied. Pneumonia, patients who started hemodialysis or peritoneal dialysis during hospitalization. A total of 123,378 patients were included before matching, including 66,692 non-COVID-19/ND patients, 54,132 COVID-19/ND patients, 1894 non-COVID-19 patients, There were 660 patients with novel coronavirus infection 19/D. After propensity score matching (PSM), the 2,136 patients were divided into his four subgroups consisting of 534 patients (Figure 1). S1).
Patients who underwent maintenance hemodialysis and peritoneal dialysis were recognized by patient care procedure coding as follows: less than 4 hours per session, ≥4 hours per session, and <5 chronic maintenance hemodialysis sessions. within hours, within 5 hours per session, or chronic maintenance hemodiafiltration or continuous peritoneal dialysis. One patient with COVID-19/D was dependent on both hemodialysis and peritoneal dialysis, and the remaining dialysis patients were on maintenance hemodialysis. She had 13 post-transplant patients, of which 7 were post-kidney transplant, 5 were post-stem cell transplant, and 1 was post-liver transplant.
Patient characteristics
Barthel Index scores at admission and discharge are calculated based on 10 functional abilities, including eating, bathing, dressing, grooming, toileting, bowel control, bladder control, chair transfer, walking, and climbing stairs. it was done.twenty one. The Barthel Index ranges from 0 to 100 points, with the highest scores indicating greater functional independence and lower scores indicating more bedridden status. Barthel Index scores were used to classify dependence into four groups: complete dependence (0–20 points), severe dependence (21–60 points), moderate dependence (61–90 points), and Mild Dependency Complete Independence (91-100 points)twenty two,twenty three. In addition, other clinical data on hospitalized patients were collected, including age, gender, BMI, dialysis dependence, and the latest Charlson comorbidity index excluding renal disease.20,twenty three, comorbidities, and type of hospitalization (urgent or non-urgent). The age groups used for analysis were 18-49 years, 50-59 years, 60-69 years, 70-79 years, and he was over 80 years old.twenty four.
result
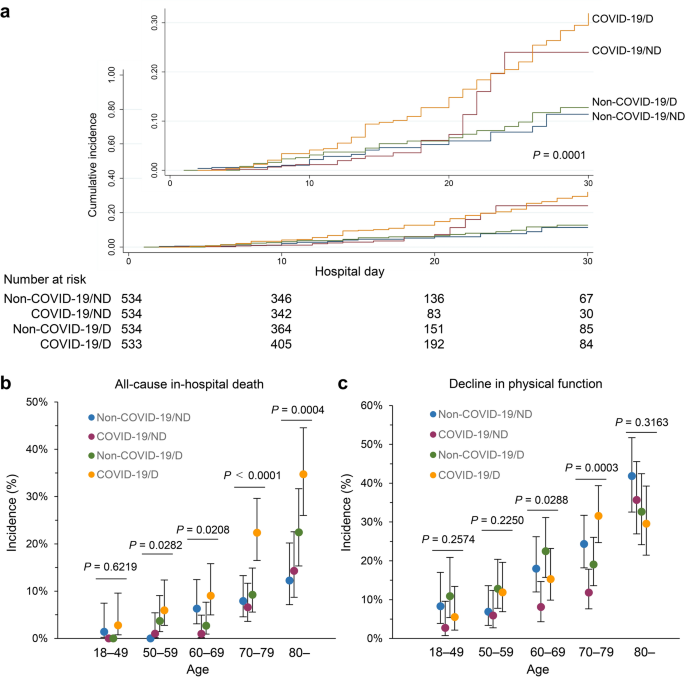
The primary outcome of this study was the occurrence of in-hospital death from any cause. The secondary outcome was decline in physical function, defined as at least a 20% reduction in Barthel Index score at discharge compared with admission. We also assessed the risk of death directly from pneumonia or from other diseases. The database identified death due to COVID-19 or non-COVID-19 pneumonia as the primary diagnosis during hospitalization, or death due to other reasons. Other outcomes include length of hospital stay and medical costs. Long-term hospitalization was defined as hospitalization for 30 days or more. High medical costs were defined as the highest quartile of participants.Patients were followed until discharge, transfer, or in-hospital death.20.
data analysis
Baseline characteristics were expressed as numbers (%) or median (interquartile range). Wald confidence intervals for the proportions were examined. Propensity scores were estimated using a logistic regression model. Differences in age (18–49 years, 50–59 years, 60–69 years, 70–79 years, and ≥80 years) and gender were adjusted to minimize potential confounding effects. Non-COVID-19/D patients (pre-matching, N= 1894; post matching, N≥534) were first matched with COVID-19/D patients (pre-matching, N==660; Post matching, N= 534). After that, the new coronavirus infection (pre-match, N==54,132; Post matching, N≥534) and non-COVID-19/ND patients (before matching, N==66,692; Post matching, N±534) was adjusted for each COVID-19/D patient. The caliper width used for matching was set to 0.25 of the standard deviation of the propensity score. The cumulative hazard after hospitalization for pneumonia was assessed using the Nelson-Ahlen estimator among the four groups. Log-rank test was used for statistical comparisons. Risk of mortality or functional decline was estimated using logistic regression analysis between patients after matching, adjusting for age, sex, BMI, Barthel Index score at admission, and Charlson Comorbidity Index score . Statistical analyzes were performed using JMP Pro 12.0 software (SAS Institute Inc., Cary, USA). p– Values less than 0.05 were considered statistically significant.
 Arabic
Arabic Chinese (Simplified)
Chinese (Simplified) Dutch
Dutch English
English French
French German
German Italian
Italian Portuguese
Portuguese Russian
Russian Spanish
Spanish